Procedures
Obstructive Sleep Apnea Surgery
Understand what OSA is, what your sleep study means, and when airway-focused surgery such as maxillomandibular advancement (MMA) or selected genial tubercle advancement may help. Care is individualized and anatomy-driven.
What is obstructive sleep apnea?
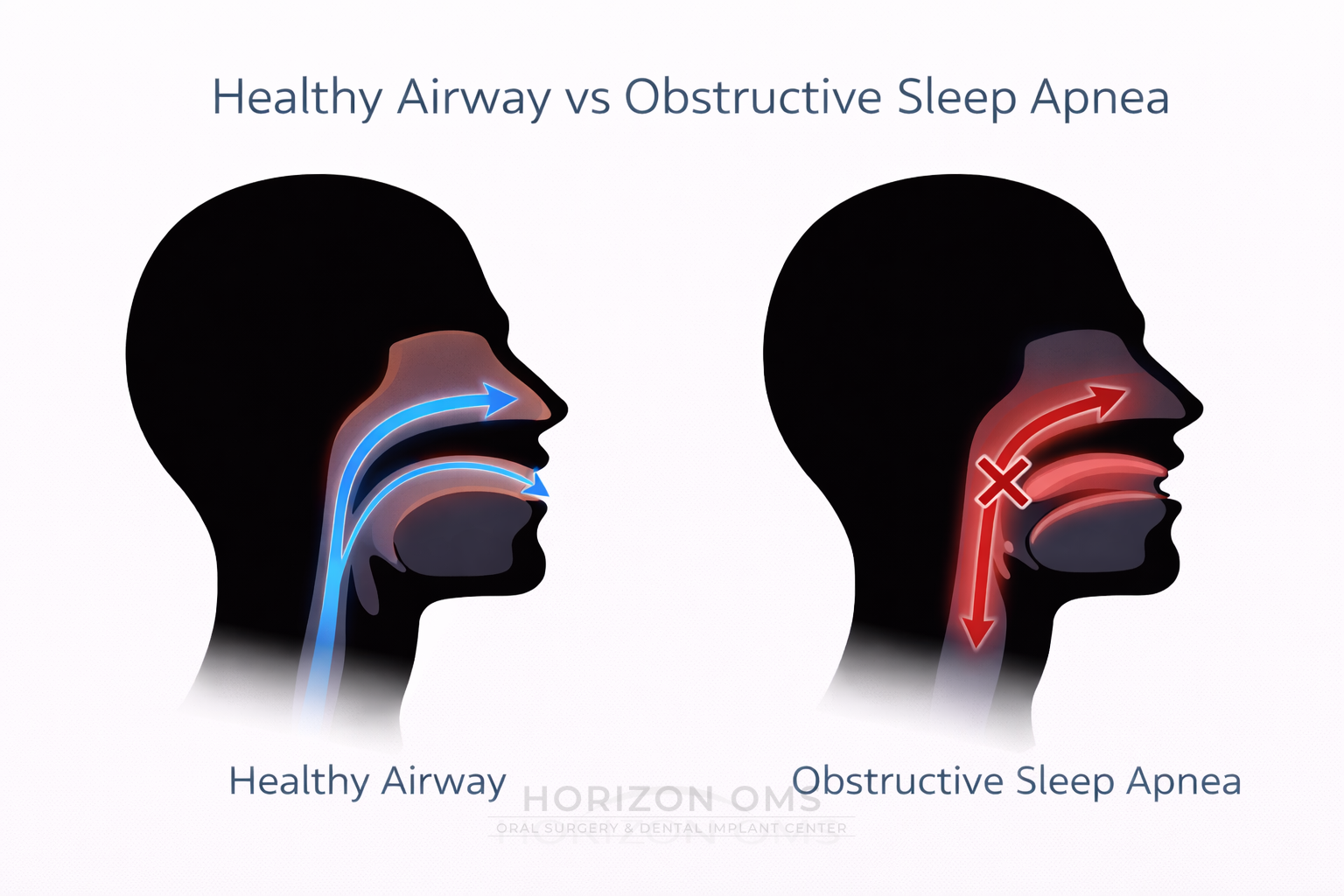
Obstructive sleep apnea (OSA) is a sleep-related breathing disorder in which the upper airway repeatedly narrows or fully closes during sleep. That creates repeated apneas and hypopneas, fragmented sleep, oxygen drops, and stress on the cardiovascular system. In plain language: the airway keeps collapsing when the body is trying to breathe.
What causes the airway to collapse?
OSA is usually not caused by just one thing. Common contributors include a narrow jaw structure, a retrusive lower jaw, a tongue that sits too far back, soft-palate crowding, enlarged tonsils in some patients, nasal resistance, weight-related airway narrowing, and sleeping on the back. Many patients have a combination of soft-tissue crowding and skeletal anatomy.
For that reason, the right treatment depends on where the obstruction is happening. In patients whose airway is limited by jaw position and tongue-base crowding, skeletal advancement procedures may provide a more definitive airway enlargement than soft-tissue surgery alone.
Common symptoms and warning signs
- Loud snoring or witnessed pauses in breathing
- Gasping, choking, or restless sleep
- Daytime sleepiness, poor concentration, morning headaches, or brain fog
- Dry mouth, sore throat, or non-restorative sleep
- Worsening blood pressure control, fatigue, or falling asleep unintentionally
How sleep apnea can affect health
Repeated airway collapse causes two major problems night after night: intermittent oxygen drops and repeated arousals from sleep. Over time, that pattern has been linked with high blood pressure, stroke, heart attack risk, atrial fibrillation, impaired attention, memory problems, mood changes, and excessive daytime sleepiness. That is why a real diagnosis and real treatment matter.
What is a sleep study?
A sleep study measures breathing during sleep. Some patients undergo an in-lab polysomnogram, while others may be diagnosed with a properly selected home sleep apnea test. These studies track breathing interruptions, oxygen levels, sleep disruption, and related data that help determine whether OSA is present and how severe it is.
What is AHI and how is severity measured?
AHI stands for apnea-hypopnea index. It estimates how many times per hour breathing either stops or becomes shallow enough to count as an event. In adults, the usual severity ranges are:
| AHI range | Severity | What it generally means |
|---|---|---|
| < 5/hour | Normal range | Not diagnostic of adult OSA by AHI alone |
| 5 to < 15/hour | Mild OSA | Real disease, often with snoring, fatigue, or sleep fragmentation |
| 15 to < 30/hour | Moderate OSA | Higher event burden and greater medical impact |
| 30+/hour | Severe OSA | Major airway event burden with greater long-term risk |
When does surgery enter the conversation?
Surgery is not the right answer for every patient, and it should follow a confirmed diagnosis and an airway-focused exam. Surgical management becomes especially relevant when:
- CPAP is difficult to tolerate or not realistically sustainable
- Anatomy shows a retrusive maxilla, retrusive mandible, or clear tongue-base crowding
- There is a dentofacial component that overlaps with corrective jaw surgery
- The goal is a more definitive structural enlargement of the airway
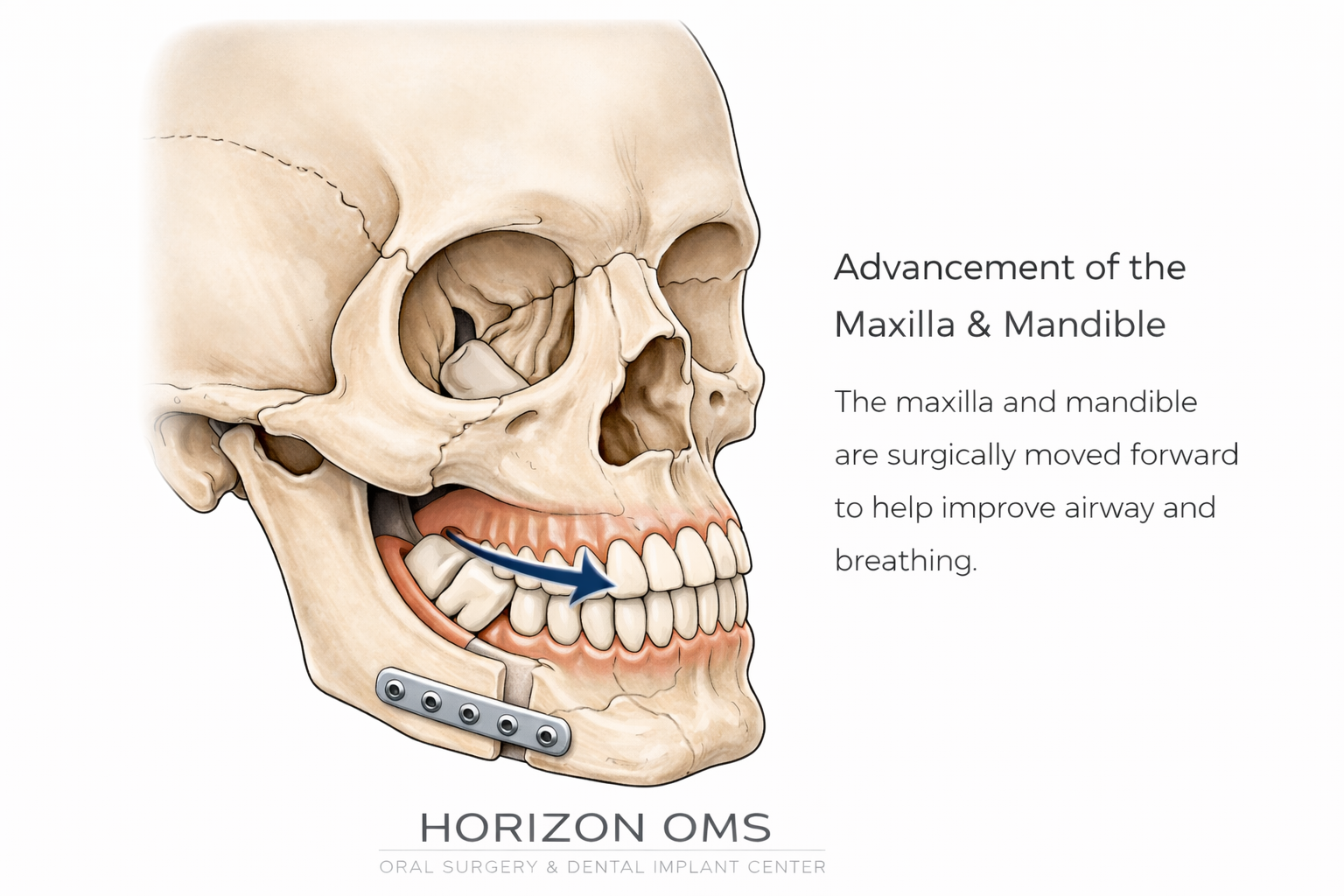
Maxillomandibular advancement (MMA)
MMA moves the upper jaw and lower jaw forward to enlarge the airway behind the soft palate and behind the tongue. In properly selected patients, it is one of the most powerful surgical options for moderate to severe OSA because it addresses the airway framework itself rather than just trimming soft tissue.
For some patients, MMA also overlaps with bite correction, facial balance, and functional jaw issues — which is why this page naturally connects with our orthognathic surgery work.
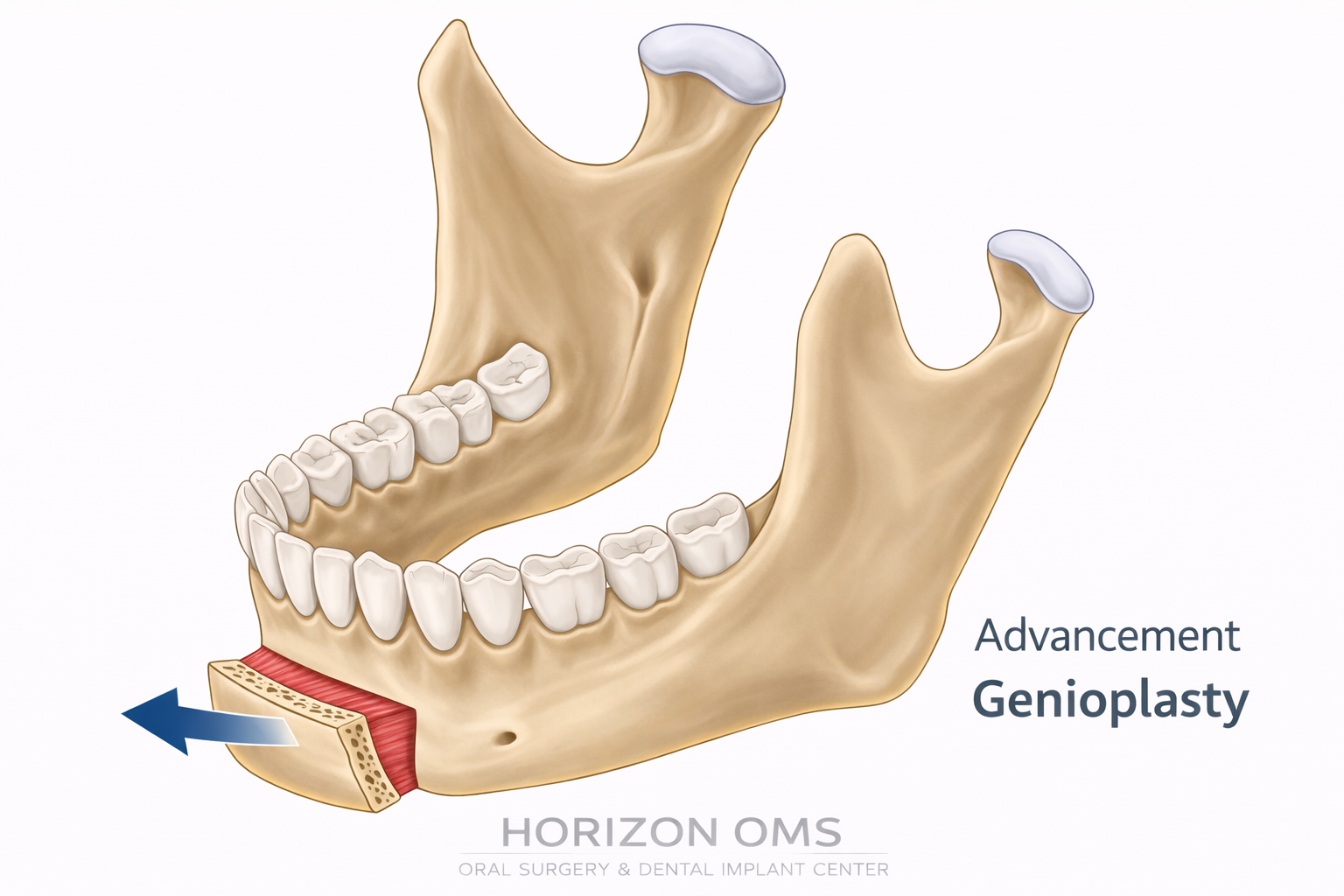
High genioplasty / genial tubercle advancement
In selected patients, a high genioplasty or genial tubercle advancement can help bring the tongue base forward by advancing the area where the genioglossus muscle attaches. It is not a universal substitute for MMA, but in the right anatomy it can be an important part of airway-focused planning.
Some patients also have other oral findings that matter during overall treatment planning. For example, large lingual or palatal tori may contribute to oral crowding, appliance issues, or prosthetic limitations and can be addressed separately when appropriate.
How effective is MMA for OSA?
MMA is one of the most studied and most effective surgeries for adult OSA. A classic meta-analysis reported a pooled surgical success rate of 86%, with the mean AHI dropping from 63.9 to 9.5 events per hour. More recent reviews continue to show that MMA has one of the highest success rates among current sleep apnea surgeries.
That does not mean every patient gets the same result. Success depends on the starting anatomy, severity, body habitus, airway pattern, and whether the procedure truly matches the obstruction pattern. The key is proper patient selection.
What happens at a surgical consultation?
- Review of your sleep study, symptoms, and prior treatment attempts
- Exam of airway-related anatomy, bite, jaw position, and tongue space
- Discussion of whether the problem appears soft-tissue dominant, skeletal, or mixed
- Clear explanation of whether surgery is reasonable, and which procedure actually fits the anatomy
Who may benefit from evaluation by an oral & maxillofacial surgeon?
Patients with moderate to severe OSA, CPAP intolerance, retrusive jaws, dentofacial deformity, or tongue-base crowding often benefit from evaluation by a surgeon who is comfortable with both airway surgery and jaw surgery planning. That is particularly true when the anatomy points toward MMA or a skeletal advancement strategy rather than a soft-tissue-only approach.