Procedures
Tooth Extractions for Patients on Prolia or Bisphosphonates
If you take Prolia, Fosamax, Reclast, Xgeva, or similar medications, extractions and dental implants may require additional planning. We’ll review your medical history and tailor a safe approach based on AAOMS guidance.
What is MRONJ?
Medication-related osteonecrosis of the jaw (MRONJ) is an uncommon healing complication that can occur after dental surgery in patients taking certain bone-strengthening medications. Most patients heal normally — our goal is to help you understand your personal risk and plan treatment safely.
Why these medications can affect healing in the jaw
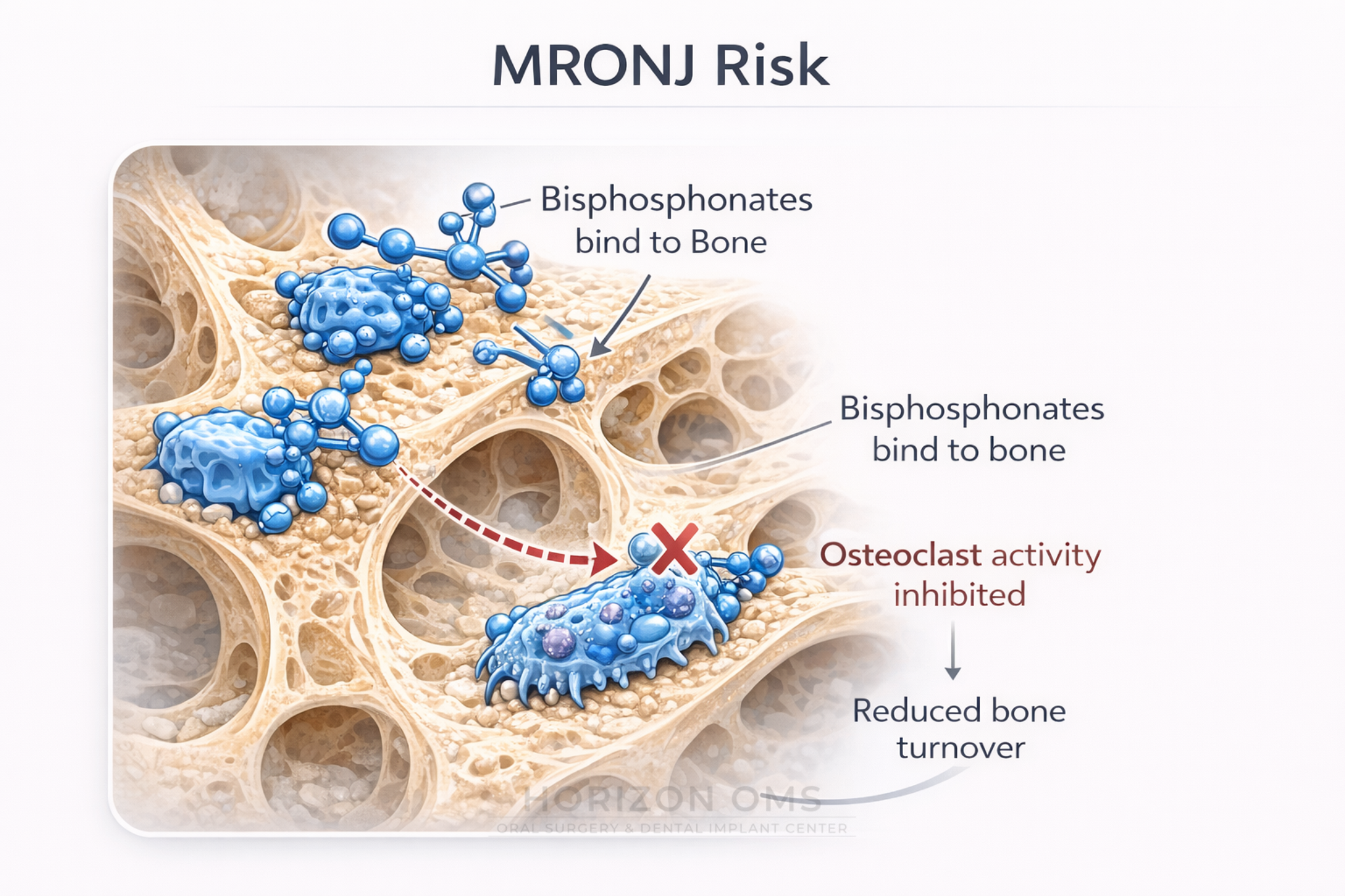
Medications like bisphosphonates and denosumab help strengthen the skeleton by reducing bone cell turnover. That’s beneficial for osteoporosis or cancer-related bone disease, but it can also mean the jawbone may heal more slowly after a surgical procedure such as a tooth extraction.
Which medications matter?
- Oral bisphosphonates (osteoporosis): Fosamax (alendronate), Actonel (risedronate), Boniva (ibandronate)
- IV bisphosphonate (osteoporosis dosing): Reclast (zoledronic acid)
- Higher-dose cancer regimens: Zometa (zoledronic acid), Aredia (pamidronate)
- Denosumab: Prolia (osteoporosis dosing), Xgeva (cancer dosing)
Osteoporosis dosing vs cancer dosing: why it changes the conversation
One of the most important details is why you are taking the medication. Patients taking osteoporosis-dose medications usually have a low absolute MRONJ risk, while patients receiving higher-dose cancer-related regimens generally require more cautious planning and closer coordination.
For example, Prolia is typically given every 6 months for osteoporosis-related indications, while Xgeva contains the same active ingredient, denosumab, but is used in higher-dose oncology regimens. Similarly, Reclast and Zometa are both zoledronic acid products, but the indication, dose, and frequency can be very different.
What we need to know before planning an extraction
Please bring or send as much detail as possible before your visit. These details help us estimate your risk, decide whether additional coordination is needed, and plan the safest surgical approach.
- The exact medication name: Prolia, Xgeva, Fosamax, Reclast, Zometa, Boniva, Actonel, Aredia, Evenity, or another bone medication
- The reason for treatment: osteoporosis, osteopenia, cancer-related bone disease, multiple myeloma, metastatic disease, or another condition
- How long you have taken it and whether it is oral, injection, or IV infusion
- Date of your last dose and, for injections or infusions, the date your next dose is scheduled
- Your prescribing physician’s name and contact information
- Whether you take steroids, chemotherapy, immunotherapy, antiangiogenic medication, or medications affecting healing
- Any history of exposed jaw bone, delayed extraction healing, radiation to the jaws, diabetes, smoking, or denture irritation
Prolia timing: do not stop or delay medication on your own
Patients often ask whether they should “skip” Prolia before an extraction. The safest answer is: do not stop, delay, or restart Prolia without your prescribing physician involved. Prolia timing can matter because stopping denosumab may increase fracture risk, including vertebral fracture risk, in some patients.
At Horizon OMS, we review the dental problem, infection level, urgency, medication timing, and medical history. When needed, we coordinate with the physician managing your osteoporosis or cancer-related care before finalizing the plan.
If the tooth is infected, waiting is not always safer
MRONJ risk is only one part of the decision. An untreated dental infection, abscess, draining sinus tract, loose infected tooth, or severe periodontal disease can also create risk. In some cases, treating the infection promptly is safer than allowing it to worsen.
Our goal is to choose the least traumatic effective treatment. If a tooth can be predictably saved, your dentist or endodontist may discuss nonsurgical options. If extraction is necessary, we plan the procedure with careful technique, infection control, closure planning when appropriate, and close follow-up.
Realistic MRONJ risk (what the numbers actually mean)
Risk varies by medication, dose, duration, and whether infection is present. Based on the AAOMS 2022 reference ranges we use for counseling, most patients on osteoporosis-dose medications remain in a low absolute-risk range, while cancer-dose regimens carry substantially higher risk over time.
| Patient category | Common drugs | Estimated MRONJ risk | Approx. cases per 10,000 |
|---|---|---|---|
| Osteoporosis – oral bisphosphonates | Alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva) | 0.02–0.05% | 2–5 |
| Osteoporosis – IV bisphosphonate | Zoledronate (Reclast) | ≤0.02% | ≤2 |
| Osteoporosis – denosumab | Prolia | 0.04–0.3% | 4–30 |
| Osteoporosis – romosozumab | Evenity | 0.03–0.05% | 3–5 |
| Cancer – IV bisphosphonates | Zoledronate (Zometa), pamidronate (Aredia) | 1–10% | 100–1000 |
| Cancer – denosumab | Xgeva | 0.7–2% | 70–200 |
Other factors can further increase risk, including antiangiogenic medications, corticosteroid use, and longer treatment duration (especially beyond 4 years).
What happens at your consultation
Your visit is designed to answer two questions: what needs to be treated and how to treat it with the lowest reasonable risk. We will review your medical history, medications, dental imaging, symptoms, and the condition of the tooth or surgical site.
- Medical review: medication type, dose, duration, cancer vs osteoporosis indication, kidney disease, diabetes, immune status, steroid use, and smoking history
- Dental review: infection, periodontal disease, tooth mobility, bone loss, sinus involvement, existing implants, dentures, and whether the tooth is restorable
- Imaging review: periapical X-rays, panoramic imaging, and CBCT when three-dimensional anatomy changes the surgical plan
- Risk discussion: what is low risk, what raises concern, what warning signs to watch for, and how follow-up will be handled
- Coordination: communication with your dentist, endocrinologist, oncologist, rheumatologist, or primary physician when appropriate
Possible surgical precautions
The exact plan depends on your diagnosis and risk profile. When an extraction is needed, precautions may include staged treatment, conservative technique, smoothing sharp bone edges, careful irrigation, soft-tissue closure when feasible, antimicrobial rinse, antibiotics when indicated, PRF in selected cases, and scheduled healing checks.
How Horizon OMS helps reduce risk
- Detailed review of medication type, dose, duration, and medical history
- Careful technique focused on gentle handling and predictable closure when appropriate
- Managing infection and inflammation before and after surgery when needed
- In selected cases, we may use PRF (platelet-rich fibrin) to support early soft-tissue healing and comfort during the first phase of recovery.
Healing follow-up and warning signs
Most patients heal normally, but patients taking antiresorptive medications should know what to watch for. Contact us if you notice worsening pain after initial improvement, swelling, drainage, bad taste, exposed bone, numbness, fever, or a socket that does not seem to be closing.
Follow-up timing is individualized. Higher-risk patients may need closer monitoring, especially if the original tooth had infection or if the medication history includes cancer-dose therapy, prolonged treatment, steroid use, or other healing risk factors.
Are dental implants still possible?
In some cases, dental implants may still be an option — but it requires a detailed, case-by-case evaluation. We’ll review your medication history, anatomy, and clinical goals to decide what’s safest and most predictable.
Why a board-certified oral & maxillofacial surgeon matters
Patients on Prolia, bisphosphonates, or cancer-dose medications benefit from specialist surgical planning and follow-up. A board-certified oral & maxillofacial surgeon is trained to assess risk, perform complex extractions, and manage healing concerns if they arise.
For referring dentists and physicians
We welcome early referral when a patient on Prolia, denosumab, bisphosphonates, or oncology-dose antiresorptive therapy may need extraction, implant evaluation, biopsy, or management of delayed healing. Helpful referral details include the medication name, indication, dose, duration, last dose, next scheduled dose, cancer history, steroid or antiangiogenic use, infection status, and current radiographs.
For urgent swelling, spreading infection, trismus, dysphagia, fever, or airway concern, patients should be directed for urgent evaluation rather than waiting for routine risk optimization.